SHOULDER DYSTOCIA
Shoulder Dystocia
Shoulder Dystocia occurs when the baby's head delivers and the shoulder ius caught behind the symphysis pubis at the pelvic outlet.
It is considered an Obstetric Emergency, because the baby's oxygen supply is compromised during Shoulder dystocia.
The importance of training for shoulder dystocia

This is a live video of proper management of Shoulder Dystocia by the AMERICAN COLLEGE OF OBSTETRICS AND GYNECOLOGY also known as ACOG.
The doctors are trained to describe the details of how they managed the Shoulder Dystocia in a manner that protects them from a lawsuit.
It is critical to protect your baby that you preserve the evidence that may contradict this at the earliest point in time. Knowing what questions to ask, and what information to gather requires great knowledge and experience.
Learn MoreRisk factors for shoulder dystocia
There are well known risk factors for Shoulder Dystocia,
The most important ones are:
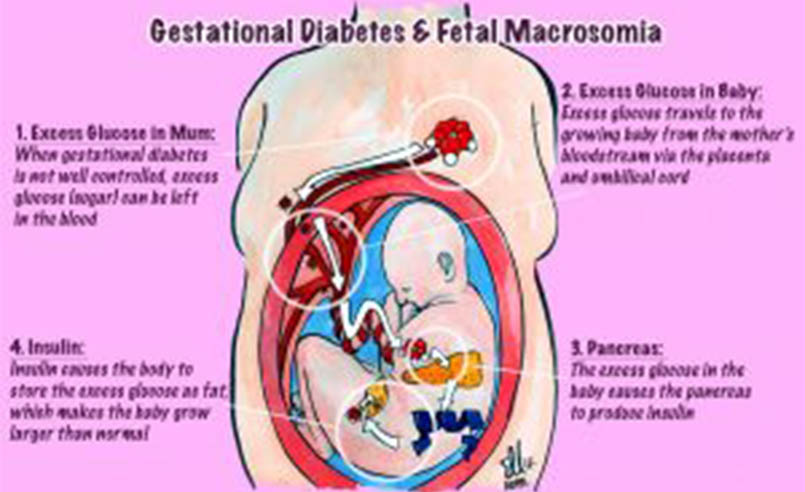
1. Macrosomia (a very large baby)

2. Gestational Diabetes. This often leads to the baby being very large, and having very large shoulders.
3. Prior Shoulder Dystocia. If you had Shoulder Dystocia in a prior delivery you are at much greater risk for Shoulder Dystocia occuring again\.
If you had these risk Factors, the doctor or midwife should have discussed a Cesarean Section with you to avoid Shoulder Dystocia.
Learn MoreArrest of dilation or dissent.
There are signs during the labor that the baby may be too large for vaginal delivery. These occur when the dilation is arrested, or takes much longer than it should, or when the dissent of the baby through the birth canal takes much longer than it should.
In addition, when the second stage of labor, which begins after you are fully dilated, takes much longer than it should, this may indicate the baby is too large for Vaginal Delivery, and he doctor or midwife should have discussed a Cesarean Section with you to avoid Shoulder Dystocia.

Management of shoulder dystocia.
The doctors or Midwife should be well trained to manage Shoulder Dystocia - but this is often not the case.
Many times they fail to even recognize or document Shoulder Dystocia. If they fail to recognize it - they are not likely to manage it properly.
Doctors should never apply downward off-axis ("lateral") force, or traction when there is a shoulder Dystocia.
The medical literature states this should be avoided at all costs.
And yet, Doctors and Midwives who are not well trained in management of Shoulder Dystocia, sometimes do exactly what they are not supposed to do.
Learn More
This causes Erb's Palsy.
Arrest of dilation or dissent.
There are well established maneuvers to relieve shoulder dystocia, which if done properly, will not injure your baby.
These include

McRoberts Maneuver:
With the McRoberts Maneuver, the mother's legs are spread apart and their knees are almost brought to touch the chest. It is intended to rotate the symphysis upward, flatten lumbar lordosis and thus increase the space in which to move the baby.

Suprapubic Pressure
Suprapubic pressure: the goal of suprapubic pressure is to decrease the fetal bisacromial diameter by adducting the anterior fetal shoulder. Pressure is applied to the suprapubic area in a downward fashion or a rocking motion from the fetal back toward the front.

Delivery of the Posterior Shoulder or Arm
Delivering the baby’s posterior shoulder works better than other maneuvers to manage shoulder dystocia when McRoberts maneuver and suprapubic pressure are unsuccessful, reports a new multicenter study published in Obstetrics and Gynecology

Wood's Screw Maneuver
During the Wood’s Screw maneuver, the clinician pushes on the posterior surface of the posterior shoulder in a corkscrew fashion in an attempt to release the trapped anterior shoulder and minimize the diameter of the shoulder girdle.
Unfortunately, when the doctor or midwife is not well trained in managing Shoulder Dystocia, they may perform the maneuvers incorrectly, and apply downward off-axis ("lateral") force, or traction.
This causes Erb's palsy.
Learn MoreWhich arm and how was it managed

Anterior Shoulder Dystocia
Almost all Erb's palsy injuries at birth are related to anterior Shoulder Dystocia.
Learn More
Anterior refers to the shoulder which is up - towards the mothers front - with the mother laying on her back during labor.
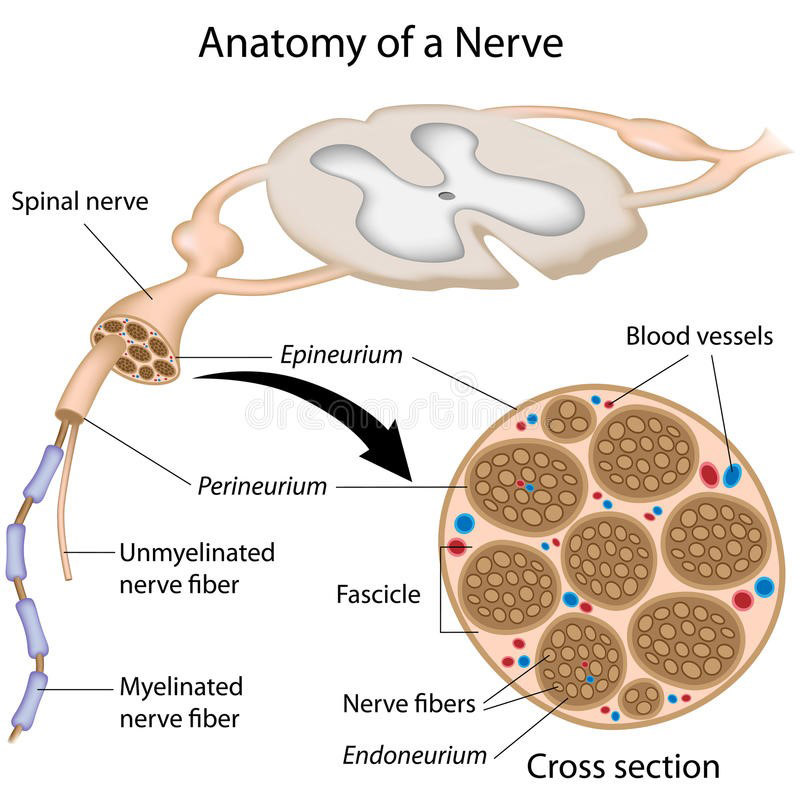
Almost all Erb's Palsy cases occur when the anterior shoulder and arm is injured during Shoulder dystocia. The shoulder becomes caught on the maternal pelvic outlet, on a structure called the Symphysis pubis. If the delivering physician or midwife applies lateral, or off-axis force or traction, they can severely stretch the brachial plexus, which is the sheath of nerves running from the spinal cord into the arms and hand.
Lateral, or off-axis traction should NEVER be applied during Shoulder dystocia. Understanding the reason for this has to do with the specific anatomy of the nerves within the brachial plexus, including their structure and direction. Researchers in France, led by Dr Metaizeau, tested still born babies to learn in the real world the structural configuration, and the impact of lateral traction upon them.

When excessive lateral traction is applied, we see not only injury to the nerves, but often to the muscles and supporting structures.




In Lawsuits, these cases are often defended by the doctor claiming that the posterior arm was injured. The posterior arm is the arm and shoulder that is closer to the mother's back as she pay on her back. The argument raised is that this occurs prior to the delivery of the baby's head, and therefore without any misconduct by the delivering doctor or midwife.
This is usually just false information that may, or may not be documented in the medical record.

Learn how to know whether your baby's anterior or posterior arm was injured.
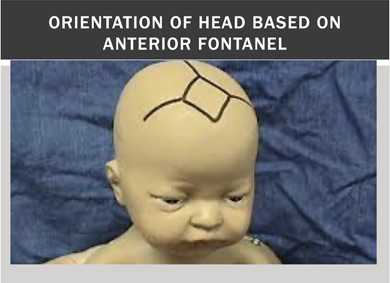
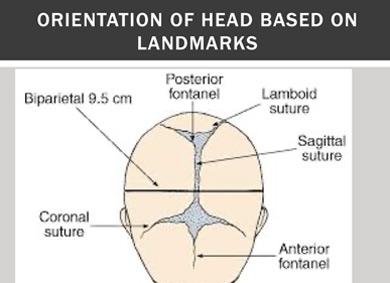
It may be on you and your family member who was in the delivery room to prove whether the injured shoulder and arm was anterior or posterior. To do this you need to understand the anatomy of the baby as it is delivered.




The direction of the head during the shoulder dystocia will tell you which shoulder was anterior and which shoulder was posterior.
You should consider speaking with an Attorney specializing in these cases while your memory is fresh.
Keeping your own record of whether the injured arm was anterior or Posterior
Sometime its hard for the mother giving birth to know whether the injured arm is anterior or Posterior. however, family or friends in the room with you can often see this. They should be asked to write down this information while their memories are fresh.
Preserving the \facts and information about what happened during the birth is critical, so contact an experienced Erb's aplsy lawyer.
Learn MoreOur Gallery